
Nutrition in Surgical Patients: Key Strategies for Better Outcomes

This podcast explores the critical role of nutrition in surgical care, discussing the impact of malnutrition, modern dietary guidelines, and approaches like enteral and parenteral nutrition to optimize patient recovery and reduce complications. Transcript Speaker 1: Hello and welcome back to Surgery 101. The podcast brought to you with help from the Department of Surgery at the University of Alberta. My name is Dr Jonathan White. I’m a general surgeon here at the Royal Alexandra Hospital in Edmonton. This is the fifth in a series of episodes all about general surgical topics. In this week we’ll be considering the topic of nutrition in surgical patients. We’ll be hearing from Dr. Leah Gramlich, who’s a colleague of mine here at the Royal Alexandra Hospital. She’ll be explaining why nutrition and malnutrition is so important in patients having surgery and looking at some of the typical guidelines for what we feed hospitalised patients. And she’ll be considering ways we can enhance nutrition in surgical patients, including oral nutrition and alternative methods of nutrition. So let’s get ready to explore the proper care and feeding of surgical patients. Here on Surgery 101. Speaker 2: Welcome my name is Lia Gramlick and this surgery podcast is about food and nutrition in your surgery patients. I’m a gastroenterologist and a physician nutrition specialist at the Royal Alexander Hospital. There are six things that I want you to take away from this short podcast. Firstly, I want you to be able to describe why nutrition or malnutrition is important in your patients. I want to be able to describe dietary components, guidelines, and food considerations in hospitalized patients. We would like to describe strategies to enhance food intake in hospital patients. We want to talk about alternatives to oral diet, including and parenteral nutrition and the rationale for the use of parenteral and parenteral nutrition indications, contraindications, and complications. Let’s begin. Malnutrition is prevalent in up to 45% of hospitalized surgery patients in Canada. Patients with malnutrition, based on the subjective global assessment, have longer lengths of stay, more perioperative complications, higher risk of death, higher costs, and poorer quality of life. This podcast will review diet considerations in surgery in patients and we’ll talk about alternatives for those patients who are unable to meet nutrient requirements by mouth. It’s important to recognize that risk for malnutrition exists and that we have a plan in place to prevent it, to detect it and to treat it so that outcome for the surgical patients can be optimized. Dietary considerations in surgery patients are unique. Dietary intake is described in the Canada Food Guide for Healthy Eating and it suggests a pattern of dietary intake that’s associated with health. It includes foods in four groupings, fruits and vegetables, grains, milk and milk products, and meat and alternatives. Taken in the right amounts, these food groups and foods provide macronutrients, protein, carbohydrate, and fat, and micronutrients, electrolytes, mineral trace elements and vitamins. Inpatients who require surgery, their underlying disease and its treatment may predispose them to malnutrition as might their hospital stay. Patients who are awaiting surgery are often kept fasting prior to surgery or for tests or they may have trouble accessing food in the hospital for a variety of reasons. They can’t reach it, they’re gone for investigations, they’re anxious. This might increase their risk for malnutrition and subsequent poor surgical outcome. Surgeons are in a great position to be aware of modern fasting guidelines. Specifically, patients are allowed to eat solids up to six hours before surgery and may have liquids up to two hours before surgery. In addition, surgeons need to be aware of that early resumption of oral intake following surgery, for instance on post-op days zero or one, should sometimes be the rule. We use commonly oral nutrition supplements like N-Sure or Boost to get calories and protein into patients who might not be hungry for regular meals or who might not be ready to take in a regular diet. One of the other ways that healthcare professionals in general and surgeons in particular can pay attention to food intake in their surgery patients is to deal with symptoms that might be a consequence of narcotic use for pain management post-op by treating ileus with things such as gum chewing or laxatives. In addition, nausea is a very common post-op complication, the treatment of which will result in better oral intake and improvement in nutritional status, ultimately resulting in improvement in outcome. In patients who are unable to meet nutrient requirements by oral intake and who are at nutritional risk might require an alternative to oral feeding, nutrition support. There are two main categories of nutrition support. Antral nutrition or feeding via tube usually through the nose into the stomach or into the small bowel. Or parenteral nutrition, nutrition that is delivered by the vein. Tube feeding or enteral nutrition is indicative for patients who have an intact and functioning gastrointestinal tract, but who are unable to eat by mouth. Examples of such patients include patients who are intubated and in the intensive care unit, or patients who have had a stroke and simply cannot swallow. Enteral products are designed to meet both macro and micronutrient requirements, and these products delivered by a fine-bore nasogastric tube go into either the stomach or more distally into the small bowel when patients can’t tolerate feeding into the stomach. Contraindications to enteral nutrition include bowel obstruction and non-functioning GI tract such as you might have with a high output gastro cutaneous fistula. Complications of ventral nutrition include intolerance of tube feeds, aspiration of tube feeds, and tube malposition. In patients who are unable to meet their nutrient requirements by mouth and who do not have a functional GI tract. Parental nutrition or nutrition by the vein can be provided. Patients with this problem have intestinal failure and this may be either short term or long term. Examples of patients who have intestinal failure include patients
The Role of Trainees and Ethics in Global Surgery

Explore how medical trainees can get involved in global surgery through research, conferences, and international electives. Learn about ethical considerations like sustainability, equal partnerships, and locally driven solutions in this evolving field. Transcript Hello and welcome back to Surgery 101, the podcast brought to you with the help of the Department of Surgery at the University of Alberta. I’m Jonathan White coming to you direct and live from the Royal Alexander Hospital in Edmonton, Alberta. This week is the third and last in a series of episodes all about global surgery brought to us by visiting surgical education elective student Betty Ibrahu from George Washington University. In this episode she will be looking at how you can get more involved with the field of global surgery. She will be considering what opportunities are out there for medical students, what opportunities are out there for residents in surgery and what are some of the key ethical concerns you may come across in the field and how do you address those. So, let’s get ready to talk about how we can get you involved in global surgery here on Surgery 101. Hi, my name is Betty and I am a third year medical student at The George Washington University in Washington, D.C. This is the third episode in a three-part series on global surgery. Today we will discuss how medical students can get involved in global surgery and some ethical considerations in the field. By the end of this podcast, you should be able to identify global surgery opportunities for medical students, discuss key ethical concerns of global surgery, discuss strategies to mitigate those ethical concerns. In the past two episodes, we have explored global surgery, a field working to improve health outcomes for all in need for surgical and anesthesia care. We have discussed the widespread need for increased access to surgery. We’ve explored the global surgery 2030 goals and the importance of developing a data driven national surgery, obstetric and anesthesia plan to meet these goals. That being said, how a trainee can participate in this field is the next important topic to address. Studies have found that trainees, medical students in particular have a strong and growing interest in global health and global surgery. As global surgery continues to grow, it follows that student participation in research, conferences, and experiential learning, like international trips, internships, things like that will continue to grow. Now, global surgery, despite being a relatively small field still, has four avenues that I have identified for medical student participation. First is the Global Surgery Student Alliance, initially established in the United States with the recent establishment of the first Canadian chapters, the GSSA is an international student-run global surgery working group. The organization was established under the premise that students are a valuable resource for the advancement of global surgery. Through their website, you can find a collection of important journal articles to read, an opportunity database for students and researchers, a list of active chapters with contact information, and more. There is also a toolkit for establishing a chapter at your school or planning a global surgery event. The second way to get involved is through research. Global surgery is an academic field with new research constantly being published. How to find a PI? Well, you could start by identifying a country or topic you feel particularly strongly about. For me, for example, as a first-generation Ethiopian-Canadian, I could pick Ethiopia. Alternatively, you could pick a subtopic in global surgery you find interesting, like capacity building or orthopedics or medical education or health systems organization. Skim articles on this topic to strengthen your knowledge while also looking for commonly occurring authors. From there, you can normally find their emails either in the journal articles or through faculty information websites. Third way to get involved is through international electives. Most medical schools offer international electives through partner universities with, generally speaking, opportunities for funding. For those looking to travel abroad, this can be an excellent starting place. While the number of institutions with surgery-specific elective varies, students can also usually arrange their own trip through a PI or at the institution in their country of interest. The fourth and final way to get involved is through conferences. Conferences serve as a great way to network with other trainees, possible PIs, and future colleagues. Here’s a very short list of conferences about global surgery or with a large global surgery track. There’s the Annual Bethune Roundtable, hosted in Canada. There’s the McGill University Health Center Conference, again, annual and in Canada. There’s the Global Surgery Student Alliance Symposia, which is an annual conference in America and there’s the Incision Global Surgery Symposium, which is annual but international. Having discussed what global surgery is and how the work is being completed abroad, it would be remiss if we did not discuss the ethics of the field. This could be a whole series of episodes alone, but I thought it would be important to briefly address some key considerations. Western medical ethics are generally built on four key pillars, beneficence, non-maleficence, respective autonomy, and justice. These pillars should, but are not always applied to global health. A 2010 article in the World Journal of Surgery outlined seven sins of humanitarian medicine. They are, one, leaving a mess behind. Two, failing to match technology to local needs. Three, failures of non-governmental organizations to cooperate with each other. Four, having no follow-up plan. Five, allowing politics to trump service. Six, going to areas where help is not needed or wanted. Seven, doing the right thing for the wrong reason. While the list may seem short, it actually distills a complex conversation about power differentials between high and lower middle-income countries into seven brief points. It highlights the importance of locally driven solutions to locally identified problems, as well as sustainability. From a research perspective, it also touches on the plethora of studies conducted in developing countries to address the
Understanding Bariatric Surgery: Procedures, Outcomes, and Care

This podcast delves into the fundamentals of bariatric surgery, exploring four major procedures—gastric band, sleeve gastrectomy, Roux-en-Y gastric bypass, and duodenal switch. Learn about patient considerations, surgical impacts, and the importance of postoperative care for long-term success. Transcript [00:00] Hello and welcome back once again to Surgery 101, the podcast series brought to you with the help of the Department of Surgery at the University of Alberta. This is Jonathan White broadcasting to you [00:20] live from the Royal Alexandra Hospital in Edmonton, Alberta. This week’s episode is number 3 in a series on bariatric surgery and obesity, brought to us by medical student Julie La, who is visiting on a surgical educational active from McMaster University. In this episode, Julie will be getting to the main topic, the bariatric surgery [00:40] itself she’ll be giving a brief overview of the four main procedures, the gastric band, the gastric bypass, the sleeve gastrectomy and the juillenal switch. So let’s get ready to get all the way up into bariatric surgery itself here on surgery 101. [01:00] Hi everyone, my name is Julie Law and I’m a third and final year medical agent. [01:20] Student at McMaster University in Hamilton, Ontario. This podcast was written and produced with guidance and support from Jenny Marshall, program assistant in digital education, and Dr. Jonathan White, general surgeon at the University of Alberta, creator of Surgery 101. The expert content reviewers were Dr. Alia Kanji, bariatric surgeon at the University of Alberta, and Dr. Renika Moti, [01:40] assistant clinical professor in the Department of Family Medicine at the University of Alberta, and medical lead for the Edmonton Adult Bariatric Clinic. The topic of today’s podcast is surgical options for the management of obesity. By the end of this episode, you should be able to describe various types of bariatric surgery, including the adjustable gastric band, [02:00] sleeve gastrectomy, row and wide gastric bypass, and the duodenal switch. Let’s start by reviewing the NIH [02:20] guidelines for bariatric surgery. 1. Age 18 to 64 2. BMI greater than 40 or BMI greater than 35 with comorbidities such as type 2 diabetes, cardiovascular heart disease, severe obstructive sleep apnea, or GERD. 3. Some contraindications include current [02:40] substance dependency, recent major cancer, untreated psychiatric illness, diseases that would make you ineligible for any surgery, if you are pregnant, have cirrhosis, or chronic pancreatitis. Most bariatric surgery is performed by general surgeons with subspecialty training in minimally invasive surgery and bariatrics. [03:00] Bariatric surgery has been evolving since the 1950s. Many groups around the world recognized obesity as a medical issue and began to try various ways to reduce the size of the stomach, the concept of restrictive surgery, rearrange the intestines to facilitate malabsorption, and then eventually a combination of both. As we learn more about [03:20] how and why bariatric surgery works, we are learning that there are a number of gut hormones that are involved in augmenting weight loss in these procedures. These procedures, while initially done open, are now almost exclusively performed laparoscopically. In Canada, bariatric surgery is covered by our Public Health Plan, which is decided upon provincially. [03:40] With that, there is variation in procedures that are covered. In Ontario, where I’m from, the Ministry of Health funds three types of bariatric surgery, all of which are done laparoscopically. The Roux-en-Y gastric bypass, the vertical sleeve gastrectomy, and the duodenal switch. In Alberta, the duodenal switch is not yet performed, but the adjustable gastric bandage. [04:00] is. Now to review the steps in anatomy of bariatric surgery. These can be tricky to follow. Honestly, reading them in textbooks repeatedly was even difficult to follow. I hope that I’ve simplified things and the slides that we provided will be a helpful tool. This might be a section that needs a few listens. [04:20] The first procedure I’ll discuss is the adjustable gastric band. The gastric band was initially approved by the FDA in 2000. Since then, hundreds of thousands of these bands were placed around the world. The principle behind this procedure is the placement of a foreign body, the adjustable gastric band around the proximal [04:40] stomach. This is then connected via tubing to a port that sits on the fascia below the skin. The port can then be accessed to inflate the band with saline or deflate the band removing saline. The adjustment is to allow for more or less restriction. The band was initially a very attractive weight loss procedure as it is minimally invasive, adjustable, and [05:00] completely reversible. Unfortunately with it were many complications that led to a large number of these bands being removed. Next the components of the Roux-en-Y gastric bypass. This procedure includes the pouch, [05:20] which is a small segment of the stomach that is stapled off. It acts as the new gastric reservoir with a much smaller volume. This will help decrease overall intake and increase the sense of satiety or fullness. Next is the bypass part, where a distal portion of the small intestine, the jejunum, is divided and then attached to the gastric pressure. [05:40] pouch. This is called a gastrostomach to jejunum jejunostomy. This is the new pathway that food will travel and it’s called the Roo Lim. Recall the physiology of obesity. One simple way to look at it is energy in versus energy out. Using a distal portion of the small intestine will [06:00] result in bypassing a large absorptial surface, decreasing the amount of energy in. Okay, now about 100 to 150 cm downstream from this new connection, the proximal aspect of the jejunum from your division is connected to a downstream part of your small intestine. Remember, this connection goes [06:20] from the bottom part of your stomach, the distal stomach, from where the pouch was stapled off, all the way down to the proximal jejunum. But as you might notice, there’s an important area stuck between the stomach and the jejunum, the duodenum.
Understanding Artemisinin Resistance: A Conversation with Dr. Charlie Woodrow

Dr. Charlie Woodrow discusses the critical challenges of artemisinin resistance, its impact on malaria treatment, and the advancements in research that aim to combat this global health issue. Transcript [00:00:00] Interviewer: This is a podcast of the Nuffield Department of Medicine. Today we speak with Dr. Charlie Woodrow about his research on artemisinin resistance. Why is artemisinin resistance a problem? [0:00:10] Dr. Charlie Woodrow: I think artemisinins are a one-off drug. They are the most effective, most rapidly acting anti-malarial that we have and they’re very safe and well tolerated. So losing them is a major problem. Artemisinins are used in all anti-malarial treatments for the main form of malaria that we see around the world, falciparum malaria, and they’re used in combination with a partner drug. But all treatments should contain an artemisinin. So once we start to lose that activity, which is what we see in resistance, we have major problems both in treating individual patients and in controlling malaria as a public health problem. [0:00:49] Interviewer: And how has artemisinin resistance developed? [0:00:52] Dr. Charlie Woodrow: So that’s a classic example of evolution. So when you treat a patient with malaria and you do not kill all the the parasites, the survivors are more likely to be resistant to artemisinin. And the reasons why that might happen relate to why treatment might fail. So, patients who don’t complete their courses, patients who just take an artemisinin without this partner drug that we need as well, and there’s also a problem with fake or substandard anti-malarials which don’t contain enough of the compound. [0:01:25] The other big factor is the immune system. So we tend to see artemisinin resistance appearing in areas where patients have low immunity, what we would call low transmission settings. So that’s outside Africa. Resistance has generally tended to appear in Southeast Asia or South America. And for artemisinins, it has been Southeast Asia because the drug has been made in China for much of its lifespan. And so, the local availability of artemisinins has been high. And so eventually, because of evolution, we see resistance developing. [0:02:00] Interviewer: How can we counter these resistance strains? [0:02:02] Dr. Charlie Woodrow: So the simple thing is to give treatments correctly. So these artemisinin combination therapies to make sure that when we’re giving them, patients are completing the courses and that their infections are being cured. We can choose the partner drug that is used in combination with the artemisinin carefully to make sure that there is still efficacy for the partner drug and that’s more slower acting anti-malarials like Mefloquine or Lumefantrine. And then in the future we have to think about other alternatives. So, when we look at infections like HIV and TB, we would always treat those with three drugs and that’s a possibility for the future of malaria, although difficult to achieve in reality. [0:02:46] And beyond that, new drugs, but there are very few available at the moment. [0:02:53] Interviewer: What are the most important areas of research that have developed in the last five to ten years? [0:02:58] Dr. Charlie Woodrow: So I think the main area of research in this field has been the documentation of artemisinin resistance in the field. There was theoretical discussion about this before, but it’s quite clear that there is artemisinin resistance in the ring stage of the parasite. That’s a certain subset of the life cycle and that that’s developed across a wide area of Southeast Asia. [0:03:21] And then more importantly, in the last couple of years, we’ve understood this form of resistance and we’re beginning to understand in biological detail what the mechanism is and that’s important for several reasons. I think the first one is just to convince everybody that it’s a major problem. [0:03:40] If you can say this mutation in a particular gene happens with artemisinin resistance, then it’s much easier than the more conceptual idea that the parasites don’t respond so well in people. [0:03:54] And then understanding the mechanism, which in simple terms is a mutation in a particular protein which is called the Kelch 13 protein then allows us to study where resistance has spread to using quite simple techniques. [0:04:12] Interviewer: Why does your line of research matter? Why should we put money into it? [0:04:15] Dr. Charlie Woodrow: Understanding artemisinin and resistance both in terms of how far it’s spread across Southeast Asia at the moment and what the mechanism is, is fundamental to understanding how to treat patients, how to treat populations and how to eliminate malaria, which is a new goal that has been promoted by funding bodies and governments across the region. [0:04:40] So I think the main issue is how do we manage malaria over the next 20 to 30 years. If we don’t understand why parasites respond well or poorly to artemisinins, that’s going to be very hard. [0:04:54] Interviewer: And finally, how does your research fit into translational medicine within the department? [0:05:00] Dr. Charlie Woodrow: So I think continuing on that idea of elimination, I think this is the new goal for control of malaria in Southeast Asia. And having the means to be able to look at how artemisinins are operating in remote areas, I think is the biggest advance in the last year. So, we can take some blood that has been stored on a piece of paper, bring it to a central lab and using fairly simple forensic techniques, which is the polymerase chain reaction, PCR, we can actually determine whether parasites from rather remote areas, for example in Myanmar, which are very difficult to access with normal clinical studies, are resistant to artemisinins. [0:05:45] So I think that’s having a big effect in terms of control programs, in choosing how they treat malaria. And we’re also seeing lots of effects in terms of how people do science. So, we work with students and researchers from areas in Myanmar and other emerging
Understanding Pyloric Stenosis: Diagnosis and Management
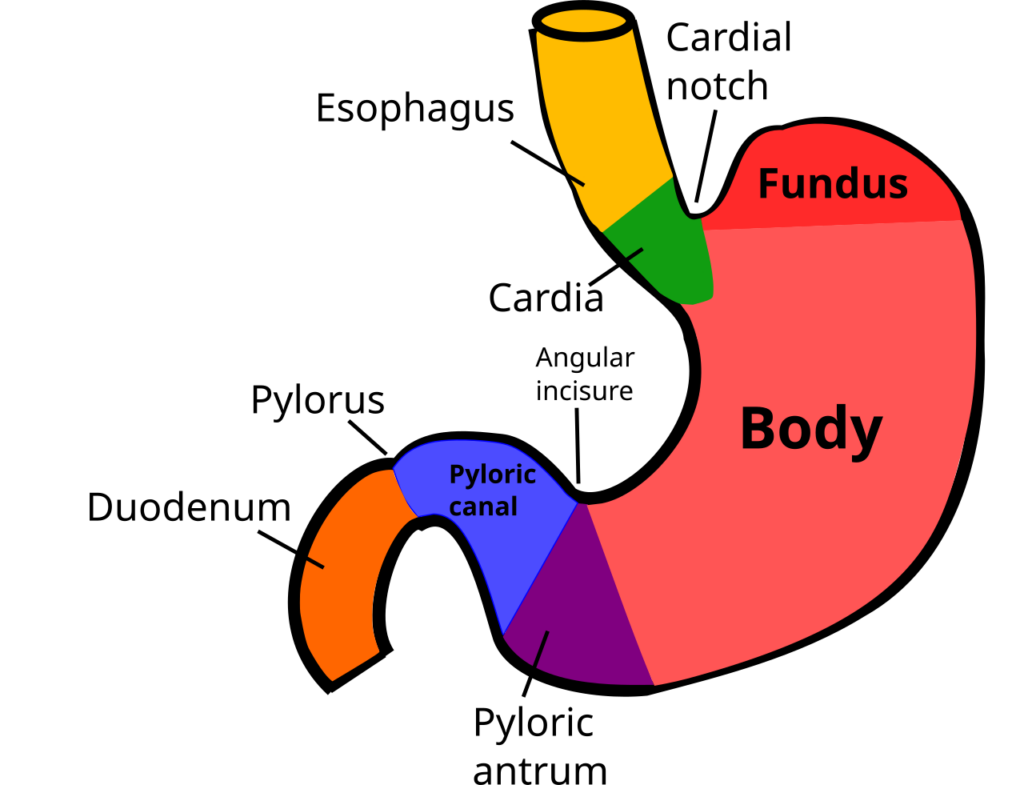
This episode explores pyloric stenosis, a common cause of gastric outlet obstruction in infants. Learn about its causes, clinical presentation, diagnostic methods, and the medical and surgical treatments to manage this condition effectively. Transcript PODCAST INTRO: Hello and welcome back to “Surgery 101”, the podcast about all things surgical brought to you with the help of the Department of Surgery at the University of Alberta. We’re available at the iTunes Music Store at surgery101.org and also at MedEd Portal. We’ve been publishing podcasts for a couple of years now and I’m delighted to bring you our 20th episode. Today we’ll be hearing from pediatric surgeon Dr. Bryan Dicken about the condition of pyloric stenosis. He’ll be telling us why you might want to know about this condition, what the cause is, how children present with this condition, and what to look for on physical examination and biochemistry. He’ll also be discussing how to make the diagnosis and reviewing medical and surgical treatment of the condition. So let’s talk about projectile vomiting here on “Surgery 101”. [00:08:06] Dr. Bryan Dicken: So to begin with, “Pyloric Stenosis”, this is an important entity to consider as it is a very common cause of gastric outlet obstruction. It occurs in anywhere between 1 in 300 and 1 in 500 live births. It has a propensity to involve males in about a 4 to 5 to 1 ratio over females and classically occurs in the firstborn male. There are some pitfalls in the diagnosis of pyloric stenosis. Most importantly is the risk of profound dehydration. Failure to thrive and even death has been reported in this entity. The particular relevance to the family physician is that there is frequently a misdiagnosis which leads to multiple formula changes which are attributed to milk intolerance or allergies. Typically, however, the pyloric stenotic child presents as a well-baby who has been feeding well up to approximately two weeks of age and then develops a sudden intolerance to feeding which is inappropriately labeled as milk intolerance or milk allergy. They typically present with vomiting and lethargy. The pathophysiology of pyloric stenosis is vague and in fact to date there is no definitive cause identified. However, there have been some putative factors such as seasonal variation, erythromycin exposure, prenatally prematurity and even transpyloric feeding tubes have been suggested as etiologies. The mechanism, however, results in hypertrophy and hyperplasia of the primary circular muscle of the pylorics and the underlying mucosa and the resultant is a partial or complete pyloric obstruction. The clinical presentation of pyloric stenosis, as mentioned, is typically a well-child that presents with non-bilious vomiting between about two and eight weeks of life. It peaks between three and five weeks of life. Having said that, there are reports of newborns as early as one day of life that have presented with pyloric stenosis. Classically it is a progressive “wet burps” which then progresses through every feed and eventually becomes classically projectile. They may have tinges of blood or coffee ground emesis associated with esophagitis or gastritis, but the child otherwise appears normal and they feed voraciously despite their vomiting. They may have diarrhea which has been referred to as starvation stools and of course this is frequently mistaken for gastroenteritis or even feeding intolerance. About 2 to 5% may present with jaundice secondary to immaturity of the Glucuronyl transferase activity as well as the dehydration associated with this condition. On physical examination there may be signs of marked dehydration such as a sunken fontanelle, dry mucous membranes and more importantly, poor urine output, as evident by a decrease in the number of daily wet diapers. In addition, the child may be found to be quite lethargic, jaundiced and a very light sign would be a decrease in skin turgor. They may have visible peristaltic waves in the upper abdomen, which is particularly marked with decompressing the stomach with an NG tube and then allowing the child a small volume of dextrose in water, which perpetuates the peristaltic waves across the upper abdomen. And more importantly, is the finding of a small palpable olive or tumor, which is classically felt at the level of the umbilicus and to the right with firm pressure downward against the spine, that the palpable pylori can be easily palpated. 80% of children will have this finding clinically. The most important finding, however, is the presence of laboratory abnormalities, which includes a hypokalemic hypochloramic metabolic alkalosis. The absence of alkalosis should make one very suspicious that it is not a pyloric stenosis. Some important differential diagnoses to include, however, would be gastroesophageal reflux disease, gastroenteritis, increased intracranial pressure from any cause, metabolic disorders, congenital causes such as Webb’s stenosis or duplications, food allergies and finally congenital adrenal syndrome. The “Treatment of Pyloric Stenosis” it is important to note that this is not a surgical emergency, but it is a potential medical emergency. It needs appropriate resuscitation prior to any consideration of the operating theater. This typically involves a fluid bolus of either normal saline or Ringer’s lactate between 20 and 40 milliliters per kilogram or until an appropriate urine output is achieved. An appropriate urine output in this particular instance would be that of 1ml per kg per hour. An NG should be placed only if there’s marked emesis, as it may perpetuate the electrolyte losses by decompressing the gastric juices. The patient should be made NPO upon suspicion of a pyloric stenosis and kept NPO until postoperatively. Labs should be measured at presentation and then at approximately 12 hour intervals until they are corrected. A corrected electrolyte profile would include a bicarbonate which is less than or equal to 25 and a potassium which is within the normal range. It is incredibly important to avoid all narcotics when treating pyloric stenosis as this tends to suppress the respiratory drive and can result in death of the infant. Rarely should patients get potassium boluses. They can be simply added to the IV solutions
Eye Health Spotlight Tackling Glaucoma with Modern Care

This episode dives into glaucoma, focusing on its types, symptoms, and management. Learn about open-angle glaucoma, acute angle closure glaucoma, and surgical and medical treatments to prevent vision loss. Transcript 00:00] Hello and welcome back to Surgery 101. The podcast brought to you with the help of the Department of Surgery at the University of Alberta. My name is Jonathan White and I’m a surgeon here at the Royal Alex [00:20] Sandra Hospital in Edmonton. This week’s episode is the second in a series of five episodes all about the eye, brought to us by medical student Kim Papp. Last week we covered the basic structure and function of the eye. This week we get to feast our eyes on the topic of blood coma. We’ll be looking at the [00:40] of the condition, the different sorts that there are and the different treatment options. So let’s get ready to think about what happens when you’ve got a little bit too much pressure in your eye here on surgery 101. [01:00] Glaucoma. Welcome to this episode of Surgery 101 on glaucoma, where we will learn the basics of this common ocular disease. My name is Kim and I am a fourth year medical student at the University of [01:20] Alberta. I’d like to give a huge thanks to Dr. Chris Rudniski for his expert review of this content. Today’s objectives are to 1. Describe the eye anatomy relevant to glaucoma. 2. Understand the pathophysiology, symptoms, and management options for open-angle glaucoma. 3. [01:40] Understand the pathophysiology, symptoms, and management options for acute angle closure glaucoma and, four, list other causes of glaucoma. Definition. Glaucoma is a common eye disease. In glaucoma, patients get optic nerve damage. Glaucoma is associated with [02:00] high eye pressure inside the eye called intraocular pressure, or IOP. Not all cases of glaucoma have high IOP, but it is safe enough for this introductory discussion to think of glaucoma as optic nerve damage with elevated intraocular pressure. The [02:20] The cutoff measurement for high IOP is usually 21 millimeters of mercury. Anatomy. How can you even get high pressure inside the eye? To understand this, we need to discuss aqueous humor and the angle of the anterior chamber. Aqueous humor is the [02:40] that fills up the anterior chamber, which is the space between the cornea and the iris. Aqueous humor is constantly being produced and drained out of the eye, so IOP can rise if aqueous is not being drained effectively. The ciliary body, [03:00] behind the iris produces aqueous humor. You may know that the ciliary body’s second job is to anchor the zonules that suspend the lens. Let’s follow the path of aqueous humor in the eye. The ciliary body produces aqueous from here, aqueous flows in [03:20] front of the lens, forward through the pupil, and into the anterior chamber. From there, aqueous drains into the angle formed by the cornea and the iris into a drainage system called the trabecular meshwork. From the trabecular meshwork, aqueous makes its way into the venous [03:40] system of the body. As an aside, if you are loving this discussion of eye anatomy and physiology, check out our other Surgery 101 podcast episode on eye fundamentals. Open-angle glaucoma. In North America, by far the most common type of glaucoma is open [04:00] open angle glaucoma. This is the type that is screened for at optometry eye exams. You may have experienced the unpleasant puff of air onto your eye when you were looking at the hot air balloon picture. This is one way to measure eye pressure, or IOP. We screen for open angle glaucoma, OAG, [04:20] because most patients with OAG are asymptomatic and because OAG causes gradual vision loss if we don’t intervene with management. What do we mean by open angle? Remember that the angle that we’re talking about here is the angle in the anterior chamber between the core [04:40] Here, aqueous humor drains into the trabecular meshwork. In open-angle glaucoma, the angle is perfectly normal and not too narrow, so the reason for the high IOP isn’t that the drainage angle is closed. So if the angle is [05:00] fine in OAG, what’s causing the high intraocular pressure? The thought here is that with age, there is microscopic dysfunction or clogging of the trabecular meshwork. So in open-angle glaucoma, aqueous humor can’t drain effectively through the trabecular meshwork. [05:20] which raises IOP and damages the optic nerve. The three major findings of chronic open-angle glaucoma are 1. high IOP, 2. optic disc changes, and 3. visual field loss. Let’s break each of these down [05:40] before diving into treatment. As mentioned before, the cutoff for high intraocular pressure is an IOP greater than 21 millimeters of mercury. For optic disc changes, ophthalmologists train to notice subtle changes in the appearance of the optic disc that signify [06:00] damage from glaucoma. One of these is a cup to disc ratio greater than 0.5. The details of this cup to disc ratio are beyond this introductory episode. For visual fields, patients with OAG tend to lose their peripheral vision slowly over time. [06:20] This is why we check their visual fields. To do this, ask the patient to look at your nose and hold out your hands midway between the two of you, holding up either one, two, or five fingers, and ask the patient how many fingers they count. Make sure they’re always looking at your nose and not taking a peek. [06:40] off to the side where your hands are. You can assess how well they see in each quadrant of vision with each eye. Let’s look at management of open-ingle glaucoma. There are many medical treatment options in the form of eye drops that are first line. These include topical prostaglandin and [07:00] beta blockers, alpha agonists, and carbonic anhydrase inhibitors. Since this podcast is with Surgery 101, however, we will focus our discussion on understanding some surgical
Understanding Unexplained Weight Loss: A Comprehensive Approach

This episode explores unintentional weight loss, its potential causes, and the diagnostic approach to uncover underlying medical or psychiatric conditions. It emphasizes the importance of targeted history, physical exams, and basic tests in patient evaluation. Transcript [00:00] Hello and welcome back once again to Surgery 101. The podcast series brought to you with the help of the Department of Surgery at the University of Alberta. I’m Dr Jonathan White. Coming to you live from the Royal Ag Center [00:20] Hospital in Edmonton. This is the latest episode in our series of episodes on general surgery. This week we’ll be hearing again from Dr. Leah Gramlich, my gastroenterology colleague here from New Orleans, Alexandria, about the topic of unexplained weight loss. And this is one of those topics that I’m afraid to say we don’t teach very well in medical school, because it’s a fairly general [00:40] presentation and it’s not necessarily connected with any one particular system. So Leah will be exploring the topic for us. She’ll be defining what is significant in terms of weight loss. She’ll be explaining what happens when you lose weight and what are some of the possible causes and she’ll be describing an approach to trying to figure out what’s happening in a patient who’s had a significant [01:00] significant amount of unintentional weight loss. So let’s get ready to investigate the case of the missing weight here on Surgery 101. [01:20] Welcome. My name is Leah Gramlich. I’m a gastroenterologist and a physician nutrition specialist and on this surgery podcast today I’m going to talk to you about approach to the patient with unexplained weight loss. There are four learning objectives in this talk. [01:40] The first is to describe significant weight loss, to discuss the impact of unintentional weight loss, to talk about the causes of unintentional weight loss, and to describe an approach to the patient with unexplained weight loss. [02:00] Weight loss is a very common problem seen by generalists whether they’re in family medicine, surgery, or in internal medicine. Patients who are overweight or obese may intentionally lose weight to improve their health. However, progressive weight loss [02:20] without trying or involuntary weight loss often indicates a serious medical or psychiatric illness. We’re going to discuss an approach to unintentional weight loss in the adult patient. Let’s start with a definition. Unintentional weight loss is also referred to as involuntary or unintended weight loss. I refer to it as [02:40] non-volitional weight loss. This term excludes weight loss as an expected consequence of treatment, for instance weight loss from diuretic therapy with heart failure or weight loss following bariatric surgery or as a result of known illness. Clinically important weight loss is often defined as a weight loss of more than 5% of usual weight over [03:00] 6 to 12 months. Involuntary weight loss of 5% to 10% of weight is potentially significant, and involuntary weight loss of over 10% of usual weight is always of consequence. The strongest independent predictors of unintentional weight loss include age, smoking, and poor self-reaction. [03:20] health. And the prevalence of unintended weight loss increases with age and is also higher amongst those with obesity, a group that’s particularly difficult to nail down the diagnosis in. Although there are many causes of unintentional weight loss [03:40] At a basic level, there are four key mechanisms. The first is reduction in nutrient intake. The second is increased energy utilization, such as in the case of fever or hyperthyroidism. The third cause is increased loss of [04:00] that might be from malabsorption or short bowel syndrome. And the fourth cause is altered metabolism. In the absence of fever or other causes for increased energy expenditure such as hyperthyroidism, in fact, weight loss is predominantly in [04:20] usually do to reduction in food intake, and you’ve got to elicit that on history. Progressive unintentional weight loss often indicates a serious medical or psychiatric illness. Any chronic illness affecting any organ system can cause anorexia and weight loss. In studies that looked at ueology [04:40] for unintentional weight loss, cancer is eventually identified as the primary cause in 15 to 35% of patients. Non-malignant GI causes count for about 10 to 20% of patients. Psychiatric causes account for 10 to 23% of patients. And in a quarter of cases, we don’t understand the cause. [05:00] Cancer is particularly of the lung, gastrointestinal tract, kidney, and prostate often cause weight loss and there are multiple mechanisms including anorexia and reduction in poor intake. The prevalence of weight loss is highest in [05:20] those with really complex cancers. Non-malignant GI tract diseases such as pepidoculcer disease, celiac, inflammatory bowel disease can also present with weight loss. And these patients often have GI symptoms including abdominal pain, early satiety, dysphasia, or oodinephasia, diarrhea, [05:40] or stioderia. They might even have evidence of chronic bleeding. In patients with psychiatric disorders, depression in particular accounts for weight loss in a third to almost two-thirds of patients with unintentional weight loss. This is more prominent [06:00] in nursing home patients and seniors. Eating disorders and other conditions such as bipolar may also contribute to weight loss in patients with psychiatric disorders. Endocrinopathies such as hyperthyroidism and diabetes contribute to altered nutrition [06:20] metabolism and both of these conditions can be associated with weight loss. Another condition we need to consider in patients who present with weight loss is adrenal insufficiency, although clearly this is less common. Infectious diseases such as HIV, tuberculosis, hepatitis C, and chronic halmuthic infections can also [06:40] contribute to non-volitional weight loss. Another area of medicine where we see non-volitional weight loss is in patients with advanced chronic diseases such as chronic cardiac, lung, or renal disease. Intercurrent illness in patients with chronic illness can also impact non-volitional weight loss. [07:00] As physicians, we also must consider social factors leading to inadequate dietary intake, such as food insecurity or the absence of enough money to buy food and
Exploring the Essentials of Anesthesiology
This episode introduces the basics of anesthesia, including its history, types, and the role of anesthesiologists. It explains how anesthesia works to make surgeries pain-free and safe using different techniques and medicines. Transcript [00:00] Hello and welcome back to Surgery 101. The podcast series brought to you with the help of the Department of Surgery at the University of Alberta and our partners at Covidien. I’m Jonathan White. [00:20] broadcasting to you from the Royal Alexandra Hospital in Edmonton, Alberta. It’s been a beautiful summer here and our summer students have been very busy making videos for Surgery 101. You may have seen a few of them already including Lego Can Meds and Lego eRAS. So more of those videos are coming out in the fall but for now we thought [00:40] we’d start an audio series, which we’ve been looking forward to for quite a while now. It’s a series of episodes focusing on anesthesia, because a lot of our listeners have gotten touched to say, well, we like what you’re doing in surgery, but is there any chance of making a podcast to cover the basics of anaesthesiology? So over the next few weeks, we’ll be introducing the topic, looking at [01:00] what anaesthesiology is and what anaesthesiologists do. We’ll be looking at how you assess a patient prior to anaesthesia and we’ll be looking at how you induce general anaesthesia during an operation. We’ll also look at local and regional anaesthetic and also consider how they manage post-operative pain. The first step of SODE in the series is brought [01:20] to us by Danica Kindretuk from the University of Saskatchewan. Danica was one of the very first students who did a Surgery 101 education elective with us. You may recall a couple of excellent episodes she did recently on cataract surgery and in this first episode of Anesthesia 101 she’ll be introducing the topic for us. She’ll be [01:40] looking at some of the history of anesthesia and looking at the scope of practice of an anesthesiologist. She’ll be defining local, regional and general anesthesia and then she’ll be talking about what is balanced anesthesia as well. So let’s let Danica get us started here as we consider anesthesiology on [02:00] surgery 101. [02:20] My name is Danica Kindrachuk. So far on Surgery 101, the team has covered a myriad of interesting topics, ranging from the bowels to the brain, along with some career guidance, health innovation, and patient [02:40] stories. Up until now, however, we’ve yet to cover the surgical journey from the other side of the drape. That’s right, today we’ll be talking about the role of anesthesia. The objectives of this podcast are to 1. Understand some history of anesthesia and [03:00] understand its importance. 2. Describe anesthesia and its scope of practice. 3. Understand the differences between and uses of local, regional and general anesthesia. 4. [03:20] List four main goals of general anesthesia and five. Define the term balanced anesthesia and explain its rationale. When the dreadful steel was plunged [03:40] into the breast, cutting through veins, arteries, flesh, nerves. I needed no injunction not to restrain my cries. I began a scream that lasted unintermittently during the whole time of the incision and I almost marvel that it rings not in my ears still. [04:00] So excruciating was the agony. I then felt the knife racking against the breastbone, scraping it. This performed while I yet remained in utterly speechless torture.” That was a quote from an early 19th century woman named Fanny Burke. [04:20] who underwent a mastectomy. The only anesthetic she received was a bit of wine to calm her nerves. She also needed seven men to hold her down during the procedure. This is a good reminder that prior to the advent of anesthesia many patients would forgo life-saving surgery [04:40] due to pain. Anesthesia is described in the dictionary as a loss of sensation resulting from pharmacologic depression of nerve function or from neurologic dysfunction. The term is also used to describe the medical specialty of anesthesiology. [05:00] As with many things in history, there is some debate over who, where and when anesthesia was first used. In the year 1800, Sir Humphry Davy wrote a paper on nitrous oxide, commenting on its capability [05:20] to destroy physical pain and remarked its potential to be used in surgery. Though cocaine was likely used as a topical anesthetic by some ancient tribes in South America, it was first isolated by Albert Neiman in 1860 and its first recorded use was in 1880. [05:40] The first public use of anesthesia was in October of 1846 when William Morton used diethyl ether on a patient with a jaw tumor at Harvard Medical School. It was also used for the delivery of Queen Victoria’s child in 1853. [06:00] Over the years, numerous new agents have been discovered and created and anesthesia has gone from a somewhat risky enterprise to a very safe endeavor. In the year 1950, the death rate from anesthesia was 1 in 1500. In 1995, this was 1 in [06:20] 250,000. So then, who are anesthesiologists today? Anesthesia as a medical specialty encompasses a broad range of activities and includes operating room management, [06:40] preoperative assessment, routine day surgery, acute and chronic pain management, resuscitation, obstetrical anesthesia, pediatric anesthesia, clinical pharmacology, [07:00] patient safety experts. It is in a nutshell physiology and pharmacology live in action. Anesthesia can be broadly categorized into local [07:20] regional and general. Local anesthesia involves the numbing of a small part of the body. The patient remains conscious. It is mainly used for small procedures where the nerves innervating the area of treatment can be easily reached with [07:40] injections, drops or ointments. Common procedures performed with local anesthesia are cataract removal, dental procedures and some biopsies. Regional anesthesia is used for slightly larger procedures or for those located deeper in the body. It is a [08:00] bit of a variant on
Short Bowel Syndrome: Insights, Challenges, and Management Strategies

This podcast explores Short Bowel Syndrome (SBS), highlighting its causes, challenges, and management strategies. It covers medical and surgical options, nutrient absorption issues, complications, and treatment advancements to improve patient outcomes. Transcript [00:00] Hello and welcome back to Surgery 101. The podcast brought to you with the help of the Department of Surgery at the University of Alberta. By [00:20] My name is Jonathan White, coming to you from the Royal Alexandra Hospital here in Edmonton. In this week’s episode, we’ll be hearing from medical student Leanne Kim, who comes to us from McMaster University, and she’ll be considering the topic of short bile syndrome. Given the topic, we’re going to try to be brief. [00:40] you’ll be considering what the syndrome is, how we recognize it, how it works, what are the prognostic factors, and how we treat it. So let’s keep it short with Short Bile Syndrome here on Surgery 101. [01:00] Hello, my name is Leanne Kim and I’m a third year medical student at McMaster University. [01:20] Today we’ll be discussing short bowel syndrome. After listening to this podcast, listeners will be able to 1. define the term short bowel syndrome, SBS for short 2. recognize SBS in post-surgical patients 3. describe the pathophysiology of SBS [01:40] 4. List prognostic factors for SBS 5. Describe the basis and indications for medical and surgical therapy for SBS What is Short Ball Syndrome and why do you need to know about it? Short Ball Syndrome is defined as the impairment and absorption of macronutrients and micronutrients [02:00] from a small bowel due to an adequate length and absorptive surface. Although SBS can result from congenital defects and surgeries in pediatric patients, today we would like to focus on post-surgical SBS in adult patients. Normal length of the small bowel is 6 meters for adults. Adult patients with a small bowel length of less than [02:20] centimeter due to surgical resection or bypass are at high risk for SBS. Intestinal failure where the patient remains dependent on parenteral nutrition is more likely when the small bowel length is less than 60 centimeters. In general, up to 50% of patients are able to be weaned off parenteral nutrition within five years of diagnosis. [02:40] as to gastrointestinal mucosa undergoes compensatory remodeling. Usually the remaining length of the small bowel can be found in the OR nuts. Patients with SBS are found to have low quality of life index, chronic fatigue associated with frequent defecation, dehydration, as well as frequent care for parent [03:00] nutrition pump can interfere with their sleep. Moreover, SVS is associated with increased mobility and high healthcare costs as well. With that in mind, let’s dive in. Let’s look at a case. You’re on neurogeneral surgery rotation and in the follow-up clinic you meet Charles. Charles is a 55-year-old patient [03:20] who is dependent on home parenteral nutrition two years after the small bowel resection from acute mesenteric ischemia. Since the resection, he has not been able to tolerate internal nutrition due to abdominal cramping, bloating, and persistent watery diarrhea. He has lost about 15 pounds. You notice on his chart that he was hospitalized a few weeks [03:40] ago were catheter-associated sepsis. As this has been greatly impacting his life, he’s here to discuss possible medical or surgical options for his parenteral nutrition dependence. What are common causes of SBS? The causes of SBS depend on the underlying condition that requires surgical resection. [04:00] In adults, most common causes are acute mesenteric ischemia, malignancy, and Crohn’s disease. In patients with Crohn’s disease, SBS may develop over a series of resection. In pediatric patients, most common causes of SBS are intestinal atresia, valvulus, and necrotizing intercalation. [04:20] clinical presentation. Postoperative ileus, which refers to a decrease in bowel motility following a major abdominal surgery, usually results within 24 hours after small bowel surgery. Usually, passing a gas or stool indicate the resolution of postoperative ileus. [04:40] Enterol feeding is initiated once the isleist resolves, though recently there was a cochlear review that enterol nutrition within the first 24 hours after lower gastrointestinal surgery is associated with shorter length of hospital stay. Once the enterol nutrition is initiated, patients at risk for SBS may experience symptoms such as non-proliferation [05:00] blood watery diarrhea with increased transit time, anorexia, vomiting, bloating, and abdominal cramping. All of these elements should be characterized further systematically on history. On physical exam, the patient may be cacti, tachycardic, and appear dehydrated from ongoing intestinal loss of fluid, electrolytes, and [05:20] It is important to do thorodomol and volume setus exams. In post-surgical patients with watery diarrhea, a few differential diagnoses should be ruled out before making the final diagnosis of SBS. If the patient is fibril, it is important to roll out intraabdominal sepsis with further investigation. [05:40] Infectious colitis should also be ruled out with stool studies to ensure that the patient receives appropriate treatment. Let’s look at the case again. Charles had an extensive small bowel resection from acute mesenteric ischemia two years ago and since then has not been able to tolerate enteral nutrition, eutopdominal cramping, bloating, and persistent water [06:00] area. What is the pathophysiology of compensatory modeling in post-surgical patients? In the post-resection phase, decrease in absorptive surface for macronutrients and micronutrients contribute to persistent osmotic diarrhea and bloating. In the following months, compensatory structural and [06:20] physiological adaptations take place to increase uptake of nutrients and fluid. For instance, the crypt, death, and villus height are increased and optimized to maximize the surface area that is in contact with the luminal content. The crypt cells undergo proliferation and differentiation to replenish the enterocytes and tereundocrine cells called the cells and [06:40] cells. Such hyperplasia of the mucosa is accompanied by the angiogenesis to ensure effective nutrient delivery via the hepatic portal system. Gross changes such as bowel lengthening and dilation also take place. Of interest, glucagon-like peptide 2, GLP2 for short, is an anti-rheumatoid hormone that